


The elephant in the room - The validity of ADHD and autism "self-diagnosis" amongst late discovered adult women
Part 1 - Why self-identification is helpful, not harmful, and we need clinician support

I asked 267 neurodivergent women, non-binary, and AFAB, what they felt were the potential benefits and harms associated with self-identification of ADHD or autism or a formal medical diagnosis.
This is part 1, addressing the elephant in the room, “Self-diagnosis”. In this article, I discuss the ethics of why I support self-identification, and I am building the world’s first strengths-based ADHD and autism self-identification service for adult women, non-binary and AFAB.
Thank you to everyone who took part in my research. I hope I have done you all justice. For anyone who missed out, I’ve included a number of self-reflective questions inviting contributions from the neurodivergent community. Please jump in with your opinions in the comments.
Seven benefits of self-identification
1. Cultivating self-awareness & self-acceptance
”[Self-identification is the] First step to acceptance - realising you were not an ugly duckling, you were a wonderful swan who had been trying to act duckling too long but actually swans are cool, they just don't fit terribly well into a duck-centred environment.”
From my discovery research with neurodivergent women, I know that most struggle with depression, low self-esteem, self-blame, shame and self-forgiveness. Late-discovered women said that claiming their neurodivergent identity and discovering more about ADHD or autism is the first step to letting go of toxic shame and practicing self-acceptance.
I believe there is a real need for a strengths-based ADHD and autism self-identification service that empowers adult women with knowledge, helps them discover their strengths and challenges, and offers positive psychology interventions that improve their self-esteem and mental wellbeing.
Q: How have self-identification and late discovery improved your self-awareness and helped you let go of shame? Thoughts in the comments.
2. Supporting anti-pathologisation & a strengths-based diagnosis
The medical model has faced significant criticism for labelling neurodivergent people as "disordered“ and giving deficit-based diagnoses. The neurodiversity movement argues that ADHD and autism are natural neurological differences, not disorders. Women who do not want to be pathologised are shunning medical diagnosis.
Being labelled as “disordered” and as having many “deficits” can reinforce negative self-beliefs that you are somehow “broken”, “not good enough”, and that you are fundamentally different to others. Internalisation of these messages can lead to increased rejection sensitivity, social anxiety and social withdrawal, as well as feelings of shame, self-blame, low self-esteem and depression.
”Self-identification means you start accessing resources to make the world less argh sooner, that's brilliant. You can work out what your needs are, make changes/request some support, and most of all, stop feeling like a useless human.”
Focusing on your strengths can buffer against depression and increase mental wellbeing. I believe there is a need for a service that supports women who want to self-identify positively as ADHD or autistic and clinicians who want to offer non-affirmative and strengths-based diagnoses.
Q: What would a strengths-based diagnosis and diagnostic report look like? Thoughts in the comments.
3. Avoiding discrimination & exclusion
Many women reported that they do not want a medical diagnosis to be recorded in their medical records to avoid potential discrimination and exclusion. Whilst the acceptance of neurological differences is increasing, ADHD and autistic people are still subject to a lot of stigma. A formal diagnosis can reportedly lead to healthcare discrimination, increased insurance premiums, and difficulties with employment and immigration.
”I’m kind of avoiding an autism diagnosis due to likely prejudice from doctors. I had a private ADHD dx for the same reason, but for me, this seems a “less heavy” diagnosis than autism, especially because you can be sectioned for having autism and I already have bipolar: I’m a tad worried I could be locked up for longer!”
Q: How do you feel about having ADHD or autism recorded in your medical records, thoughts in the comments?
4. Current global wait-crisis for diagnosis
”Diagnosis takes FOREVER - so it skips the necessity to wait for a medical diagnosis.”
There is currently a global wait crisis for a medical diagnosis of ADHD or autism. In England alone, over 200,000 adults are waiting for an autism diagnosis. Recent statistics from the Royal College of Psychiatrists estimate that 196,000 adults are awaiting an ADHD diagnosis across the UK. Women who were overlooked during childhood now face long waits for an NHS diagnosis, which can take several years.
”This is, in my mind, the wrong question. The point is, why should we have to self-identify? If there were enough resources, then the waiting lists would be shorter, and we could all be medically-diagnosed.?”
Long waits for a medical diagnosis can cause crippling anxiety and have a negative impact on women’s mental health. What if you could get answers in minutes? From ambiguity and uncertainty to clarity and relief. I believe that supporting self-identification has the capacity to improve women’s mental health and reduce pressure on our health system.
It is foreseeable that if we empower women to self-identify who do not want to be pathologised or want access to ADHD medications, this might give them closure and the insight they need without a medical diagnosis. In turn, the service has the potential to reduce, as opposed to increase, the demand for diagnosis and current wait time.
Additionally, the service, which generates an evidence-based narrative PDF self-report, can be built on by clinicians, expediting assessment and report writing times and potentially reducing current wait times. This has the potential to increase diagnostic accuracy and reduce missed misdiagnosis and gender bias in diagnosis.
Q: How else might we reduce the diagnosis waits and expedite the assessment and diagnostic process? Thoughts in the comments.
5. Unaffordable costs of a private diagnosis
Women who were missed in childhood and who are desperate for answers are being forced to pay up to £3000 for a combined private medical diagnosis. Many women who are marginalised simply cannot afford these costs.
A preliminary face-to-face screening with a clinician typically costs around £250 to £300. I believe clinician time could be better used to diagnose the backlog of women and that we should empower women to self-screen before pursuing a medical diagnosis. Offering a low-cost self-identification service could save women money and clinicians time conducting pre-diagnostic screening.
What if there was an inexpensive alternative that took a fraction of the time? What would you choose? What are your thoughts in the comments?
6. Supporting self-advocacy - accessing workplace accommodations & financial support
The Equality Act 2010 protects people with disabilities, including those who do not have a formal diagnosis. The Act requires employers to make reasonable adjustments for employees with disabilities.
UK government services such as Access to Work and Personal Independent Payment (PIP) continue to accept self-identification, enabling women to access financial support and the costs of services that can help with managing a disability. Access to work, for example, offers up to 69K in support. Many women are not aware of this. It will be important for the service to signpost women to these services after self-identification.
Neurodivergent women reported that they struggle with asking for support and asserting their needs, and mask their difficulties in order to fit in. I believe there is an opportunity for a service that helps women communicate their unmet needs and self-advocate. It is difficult to apply for support or ask for what you need if you are unaware of how ADHD and autism create challenges and what constitutes reasonable adjustments. It will be important for the service to offer guidance on workplace adjustments and effective communication.
Q: What signposting and support would you like to see? Thoughts in the comments.
7. Increasing connection & finding your tribe
Many neurodivergent women report childhood bullying, workplace bullying, discrimination, exclusion and social isolation. Self-identifying as ADHD and autistic can help you start to find your tribe and build your circle of support. But many women don’t know where to start. A common complaint about medical diagnosis is that women are left with no signposting to post-discovery support.
”[A] potential harm in a [medical] diagnosis is no support afterwards. Most of the time, you get a diagnosis and they are done with you. So you're left confused and vulnerable.”
An important opportunity for the service will be signposting to relational support. Being a member of a group has been shown to buffer against loneliness, stress, anxiety and depression. Prosocial coaching is a positive psychology experiment designed to widen access to positive psychology coaching for neurodivergent women, non-binary and AFAB, and tackle loneliness, social anxiety, rejection sensitivity and depression.
Prosocial coaching helps women who do not have employer or government funding or who are facing financial hardship access low-cost group coaching that will boost their confidence and mental wellbeing and grow their network of support. The groups are an opportunity to unmask, be your authentic self, explore problems experienced by neurodivergent women and experience acceptance.
To join the waitlist, email
leanne@wearemorehuman.co.uk
Potential harms with self-identification
When discussing anything related to ethics, it is important to consider and mitigate potential harms. Women really struggled to come up with reasons why supporting self-identification might be harmful and why I should cancel this project.
”The only scenario where I can envisage this being problematic is if it is inaccurate and could hold someone back from seeking an accurate diagnosis and potentially support for a different condition.”
”If self-identification has harm, I'd love to know. I have never met anyone harmed by it or who regretted it in all my over 15 years of advocacy. No one ever complained of being damaged by it to me. So, if it's happening, I'm going to guess it's a rare thing. I'd love for someone to point to a real example of someone meaningfully being harmed by someone else self-identifying or themselves being harmed by it.”
” It could be harmful if they self-identify with something that might not be correct or be the whole picture, and then they could end up missing out on finding a correct diagnosis and seeking relevant information and help.”
Perhaps I should have posed the same question to clinicians. Or the media. They have plenty to say about “self-diagnosis”.
The Daily Mail

The Telegraph
BBC News
Addressing the elephant in the room - Inaccurate self-diagnosis
"The elephant in the room" is an idiom that refers to an obvious problem that people avoid discussing openly. According to cited experts, “Too many young people are “self-diagnosing” with ADHD after viewing TikTok videos containing misinformation.” Let’s talk about that.
”People cannot just diagnose themselves.”
Through my early discovery research, I found it is largely the media and medical professionals who are using the term “self-diagnosis” and who continue to invalidate those unable to access a medical diagnosis or who actively oppose pathologisation. The same medical professionals who missed or misdiagnosed 80% of women in childhood…
This sounds a lot like a psychological projection to me. Psychological projection is when someone unconsciously attributes their own unwanted feelings or traits to someone else. It's a defence mechanism that helps protect the ego from acknowledging uncomfortable emotions.
Q: Is a medical diagnosis any more reliable or valid than “self-identification”? Thoughts in the comments.
The term “self-diagnosing” is seldom used by neurodivergent women who “self-identify” as AuDHD, ADHD or autistic. In my research, I found that they use identity-first language promoted by the neurodiversity movement and the argument that ADHD and autism are differences, not disorders. What language do you use, or did you use, prior to getting a medical diagnosis? I’m curious.
That being said, only a healthcare professional trained in diagnosing neurodevelopmental conditions can make a formal medical diagnosis of ADHD or autism. Anyone can, however, self-identify as ADHD or autistic and claim their neurodivergent identity. Women are not self-diagnosing; they are clearly self-identifying. Given that, I think we need to encourage the use of “self-identification” and promote neuroaffirmative language.
The bigger question is, why do healthcare professionals object to self-identification? Ethically, what harm could come from empowering women to self-identify ahead of medical diagnosis? Why are women not trusted in their self-reports, self-assessment, judgement or intuition? Why are we continually being dismissed and invalidated?
“I am strongly pro well-researched self-identification, as it's often a necessary initial part of the diagnostic process.”
Emphasis on “well-researched.” ADHDers have a love of learning and a thirst for knowledge. Autistic women, especially, are excellent researchers and evidence-based decision-makers and have an intolerance for misinformation. Whilst evidence-based articles about female ADHD and autism are sadly lacking (why I started She’s Opinionated), I can assure you that these women are not diagnosing themselves using TikTok. Self-discovery typically involves extensive research and a desperate search for answers. Am I wrong - how did you go about self-identifying that you are ADHD or autistic?
Whilst I don’t agree with clinician or public concerns about the inaccuracy of “self-diagnosis”, what I do agree with is that there is a desperate need for an evidence-based self-identification service that helps adult women, non-binary and AFAB self-screen for ADHD and autism, which references both the diagnostic criteria and the latest research about how each condition presents in women (Fellowes, 2024). I am working on it…
As we make progress towards launching the service, my biggest concern is ensuring validity and building a trustworthy service. To date, we have conducted two rounds of validation testing, with more validation testing coming. The service in development has been co-designed, tested and validated with 267 medically diagnosed and self-identifying women from around the world. Additionally, the service has been clinically validated and coded according to the diagnostic criteria by a clinical expert (Dr Hannah Hayward, a diagnostician who holds the first PhD in female autism). Thanks, Hannah! So, I am quietly confident it can accurately detect ADHD or autism.
That said, I also agree with concerns that there is a risk that a person may overlook the possibility of other co-occurring conditions that might better explain their traits or symptoms, preventing them from seeking treatment. ADHD and autism have an incredibly high psychiatric co-morbidity rate - so it is unlikely that a person is just ADHD or autism. So, it should be important that the service raises awareness about commonly co-occurring conditions - specifically CPTSD, depression, anxiety and PMDD.
Another common assertion is that a person with PTSD/CPTSD may wrongfully conclude they have ADHD because the two conditions have similar symptoms. I would argue that a far more likely scenario is that ADHD women may have been misdiagnosed with BPD by medical professionals instead of CPTSD, overshadowing underlying ADHD. CPTSD is significantly elevated amongst ADHD and autistic women. We should be screening traumatised women for ADHD and autism!
ADHD is associated with elevated rates of childhood abuse, intimate partner violence (both physical and sexual) against women, and the perpetration of intimate partner violence (Arrondo et al., 2023). Alongside childhood trauma, male gender, and callous-unemotional traits, ADHD is considered a criminogenic risk factor. It is estimated that at least half of the prison population has ADHD.
Neurodivergent women are more likely to be re-victimised as adults through intimate partner violence. The rate of relational trauma and victimization among women with ADHD is so alarmingly high that it would not be outlandish to anticipate that many women who develop Borderline Personality Disorder (BPD) or Complex Post-Traumatic Stress Disorder (CPTSD) due to abuse may also screen positive for underlying ADHD. This is why I want to ensure that the screening service I am building is accessible to women who are seeking support through domestic abuse, rape crisis, and homelessness charities.
There are a couple of other possible “misdiagnosis”…
”If it means you miss another important diagnosis... My daughter was believed to be autistic (she probably is), but that meant they didn’t recognise that she had schizophrenia until the point where she was very sick indeed.”
There is a huge overlap between certain conditions. For example, people with schizophrenia have both the “negative symptoms” that are seen in autistic people and the “positive symptoms” associated with psychosis. Similarly, people with Bipolar have many symptoms associated with ADHD with the addition of mania. Both psychosis and mania have such negative effects it is fairly unlikely a woman would not have already sought medical help.
This all said, schizophrenia is a common misdiagnosis for female autism, and bipolar disorder is a common misdiagnosis for female ADHD, and they frequently co-occur. Arguably, women are more likely to have been overlooked or misdiagnosed with either condition by medical professionals. Dr Neff at Neurodivergent Insights offers really excellent discussions of the overlaps through her misdiagnosis Monday series. Please do check out her infographics:
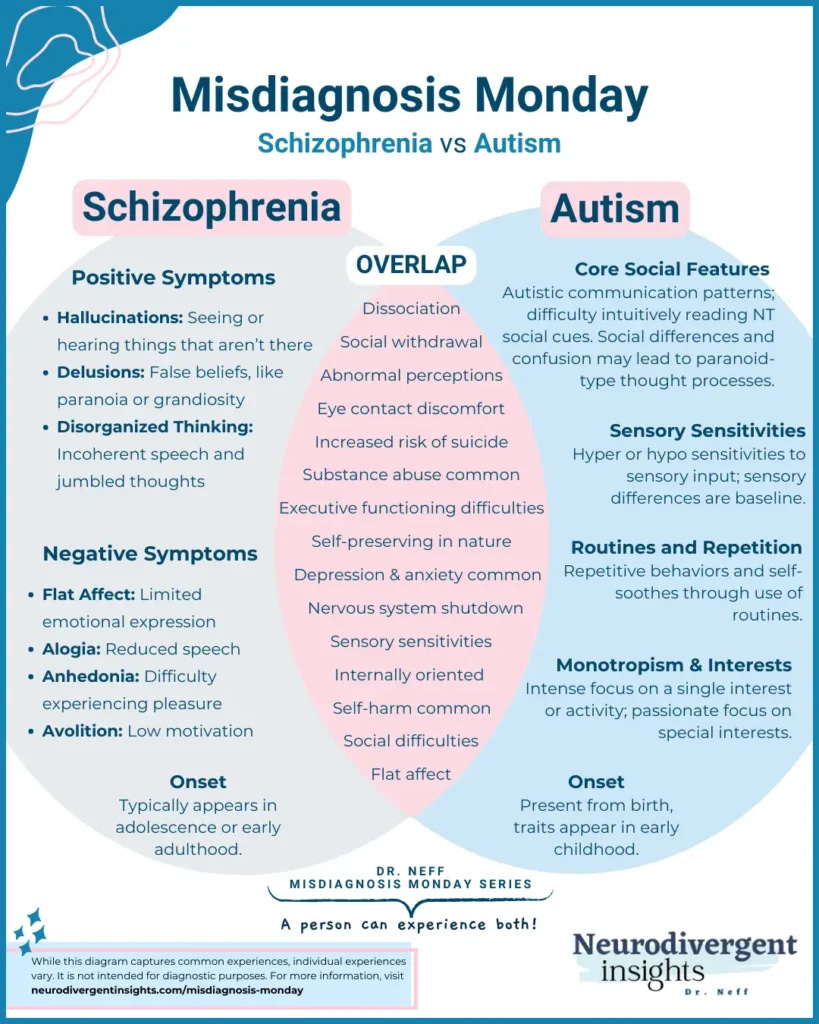
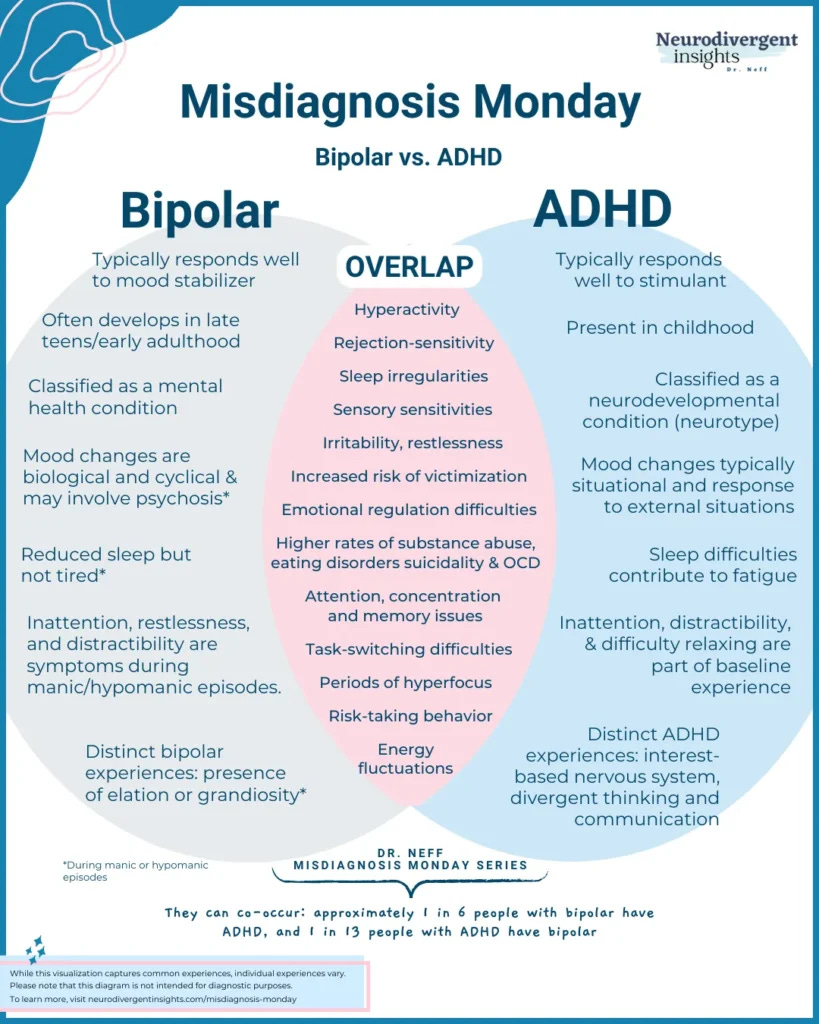
Image credit Neurodivergent Insights.
Women felt that invalidating self-identification was more harmful than choosing to support it. They believed that concerns about women misidentifying as being ADHD or autistic were largely unfounded, serving only to maintain systems of oppression and power inequity and to continue to restrict access to support.
”I have never seen anyone speak to [harm of self-identifications] anywhere ever, other than melodramatic Karens clutching pearls about it who aren't themselves affected in any way but feel the need to defend and gatekeep diagnosis in an attempt to "protect" disabled people or "prevent fraud" as if that is a common occurrence (clue, research says it is not).”
Whilst clinicians might argue that women lack the knowledge or training to “self-diagnose” with ADHD or autism, neurodivergent women might equally argue that clinicians have been “gaslighting” and misdiagnosing them for decades. At the risk of making enemies, I believe clinician criticisms of “self-diagnosis” are a clear projection of the medical profession’s failure to accurately diagnose neurodivergent women in the first place and rising insecurity in response to the rejection of pathologisation, the wave of self-advocacy and AI.
”[Self-identification is] Super important for communities that are ignored by medical professionals, women being one of them. If it wasn’t for my self-diagnosis, I wouldn't have reached a medical diagnosis. No doctors ever believed me, and nobody around me thought I was right. Self-diagnosis is key in many medical diagnoses.”
Women do not deserve to continue being dismissed and invalidated by medical professionals; we have been through enough. These women have grown up surrounded by ADHD and autistic family members their entire lives and have had more exposure than any clinician. ADHD and autism are, after all, up to 90% heritable. It is about time we find where all the missing girls and women are.
”Self-identification can be liberating and provides answers, while medical diagnosis can be necessary for accommodations. The only harm that could come up is when a medical practitioner is unkind and not empathetic, denying much of self-reported experiences.”
To that end, I am calling on medical professionals to start listening to women’s stories, elevating neurodivergent voices and supporting self-advocacy. For a thorough review of the likely accuracy of self-identification within psychiatric diagnosis, I would encourage you to read this excellent medical paper.
About the author
Hello, I am Leanne. I am a late-diagnosed neurodivergent (woman!), Positive Psychology Coach, and the founder of More Human. More Human is on a mission to close the gender gap in ADHD and autism recognition and diagnosis, widen access to good support, and create equal opportunity.
More Human are launching the first strengths-based ADHD and autism self-identification service for ADHD and autism in adult women, non-binary and AFAB. Over the past several months, I have been working with what is now 267 neurodivergent women to conduct research into their lived experience, co-design, and test a breakthrough service. As a brave survivor diagnosed with CPTSD, I feel privileged to lead this work.
I need your help to keep going.
3 ways you can support my work and help me deliver this breakthrough service
Restack and reshare this post (it is free)
To support my research and writing, upgrade to become a paid subscriber
Book 1-1 positive psychology coaching with me - see my LinkedIn references. I’m awesome. (UK funding is available through Access to Work)
Thank you for your support.
Leanne.